01
May

1. Improper acclimatization poses many problems for climbers, and facilities and supplies may be inadequate to treat all victims. Mountain sickness and other illnesses may also occur. Evacuation of the sick and wounded is compounded by the terrain and weather. In harsh mountain weather, the most important course of action is to provide first aid as early as possible. These are basic guidelines you are advised to follow under the supervision of a medical expert.
2. In consideration of the need to prevent/reduce the occurrence/severity of acute High Altitude Illness (HAI), and the existing topographical, logistic, and operational constraints, we practice a staged ascent schedule in high altitude. This is referred to as the "acclimatization schedule". However, "staging schedule" is a better term since acclimatization carries on for weeks after arrival at high altitude. The value of the Staged Ascent schedule employed by the Armed Forces has been proven over more than three decades of use, with considerable lowering of medical cases.
3. The ideal staged ascent schedule as followed by Armed Forces is as follows-
(a) Stage 1: This is applicable to individuals arriving at heights between 2700M to 3600M (9000 feet-12000 feet). The staging period is 6 days as under:-
(i) climbs. First and Second day. Rest, except for short walks only, not involving any
(ii) Third and Fourth day: Walk at slow pace for 1.5 to 3 km. Avoid steep climbs
(iii) Fifth and Sixth day: Walk up to 5 km, and climb upto 300M at a slow pace.
(b) Stage 2: On ascent to altitudes above 3600M and upto 4500M (12000 feet 15000 feet) (b) after completion of Stage 1. This is carried out for 4 days as under:-
(i) climbs. First and Second days: Slow walk for a distance of 1.5 to 3 km; avoid steep
(ii) Third day: Slow walk and climb upto 300M.
(iii) Fourth day. Climb 300M without equipment.
(c) Stage 3: On further ascent to altitudes above 4500 m (15000 feet), after completing stages 1&2 of ascent protocol. This also lasts for 4 days and is on the same lines as second stage.
Hypothermia is when the body gets very cold and cannot warm up on its own. The normal body temperature is 98.6 degrees Fahrenheit. Hypothermia occurs when it drops below 95 degrees Fahrenheit. With severe hypothermia, the core body temperature can drop below 86 degrees.
Health issues and certain medications can affect the body's ability to regulate itself when cold. Medications which affect thermoregulation include:-
(i) Sedatives or sleeping pills.
(ii) Tranquilizers (benzodiazepines) such as lorazepam.
(iii) Antidepressants, antipsychotics.
(iv) Some heart drugs including beta blockers and clonidine.
| Temperature | Stage | Symptoms |
| 97 to 99 F (36.1 to 37.2°C) | Normal body temperature | |
| 90 to 95°F (32 to 35°C) | Mild hypothermia | Shivering, goose bumps, bluish skin, confusion, trouble speaking, memory problems |
|
82 to 90°F (28 to 32°C) |
Moderate hypothermia | Shivering stops, sleepiness, seeing things that aren't there (hallucinations) |
| Less than 82°F (28°C) | Severe hypothermia | Stiffness, Loss of consciousness or coma, breathing stops, heart stops |
(i) Eat a healthy meal, which will provide enough calories to generate heat in the environment.
(ii) Eat snacks periodically to maintain calorie levels.
(iii) Have warm non-caffeinated beverages.
(iv) Do not sit on cold items.
(v) Keep moving as much as possible.
(vi) Wear appropriate clothing for insulation.
(vii) Keep clothing dry.
(viii) Cover Mittens, gloves, hats, scarfs, and ski masks, help you keep your body heat intact.
(i) Move the person to a warm, dry shelter, as soon as possible.
(ii) Remove any wet clothing.
(iii) Protect the person against wind, drafts, and further heat loss with warm, dry clothes, and blankets.
(iv) Begin rewarming with extra clothing and warm blankets.
(v) Hot packs or heating pads should be avoided as these can cause burns to the skin.
(vi) Take the person's temperature, if possible.
(vii) Offer warm beverages if the person is able to drink.
(viii) Avoid alcohol and caffeine, which speed up heat loss.
(ix) Do not briskly rub or massage the person's extremities as with severe hypothermia; this muscle activity can cause the heart to stop. Strenuous muscle activity should also be avoided.
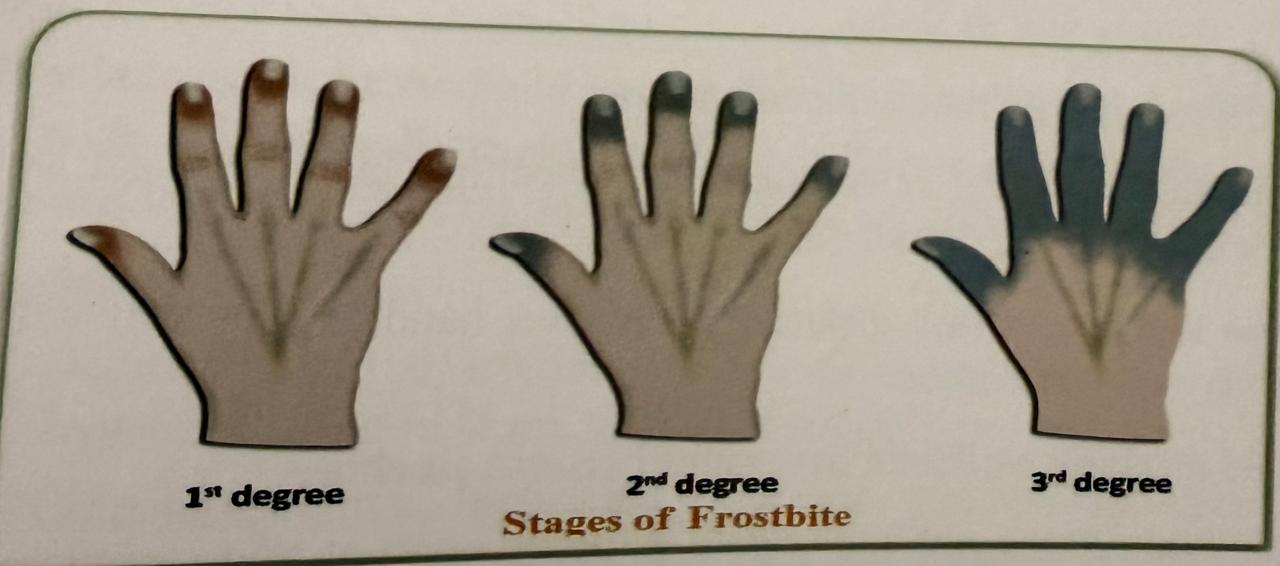
Frostbite occurs when tissues freeze. This happens because in cold weather, the blood vessels become narrow, which reduces the blood flow and oxygen to the tissues. Frostbite usually affects body parts that are farther away from the body core, and therefore, normally, have less blood flow. These include your feet, toes, hands, fingers, nose, and ears.
(i) The areas affected feel cold and firm.
(ii) Sensations of burning, tingling, stinging, or numbness.
(iii) Clumsiness can occur due to loss of motor control.
(iv) When the affected body part is rewarmed, a throbbing or burning pain may be felt
(1) Frostbite requires immediate treatment, ideally in a medical facility. Before transporting to a medical facility, the affected area should be gently and loosely wrapped by a dry sterile bandage, or clean blanket, to prevent further trauma.
(ii) The most effective treatment is rapid rewarming, which may be accomplished by immersion of the affected area in a tub of lukewarm water, that is between 40-42°C, for 20 to 40 minutes or until thawing is complete. Warm wet packs can be used if a tub is not available.
There are some conditions that occur without freezing the skin. These include chilblains, trench foot, and frostnip.
Chilblains. occur due to an abnormal vascular response, several hours after the area that was exposed to the cold is re-warmed. Persons are more at risk for getting chilblains, if they use nicotine or other drugs, that reduce blood flow to the extremities.
(i) Itchy, painful, reddish or purplish areas of swelling, usually affecting fingers, toes, nose, or cars.
(ii) Blisters or small open sores may develop, symptoms that last for several days,
(iii) After healing, the area may be very sensitive to cold in the future.
Trench foot is named after the condition suffered by soldiers in the trenches during World War I. It develops after a prolonged exposure to a wet, cold environment, and is more serious than chilblains. Tight fitting boots or shoes can exacerbate the condition. Trench foot does not require freezing conditions, and can occur at temperatures up to 15°C.
(i) Itching.
(ii) Numbness.
(iii) Swelling
(iv) Red, blotchy skin or blue-black with advanced injury.
(v) Blister and open sores can develop.
(VI) With severe trench foot, the tissue dies and falls off. Gangrene can develop and the foot may need to be amputated
Frostnip occurs in mild by cold weather, and usually affects the face, ears, toes, and fingers. Symptoms appear after exposure to cold weather.
Pale appearance of the skin.
(i) Burning, itching or pain.
(ii) Tingling and numbness.
(iii) Treatment Simple rewarming restores the normal color, and sensation, with no permanent tissue damage,
Cold injuries can be prevented, if you are prepared when out in cold weather.
(a) Avoid staying out in the cold for long periods of time.
(b) Dress warmly and in layers.
(c) Head for a shelter, that will protect from wind or rain, if you are wet or cold.
(d) Avoid activities that cause increased sweating; increases heat loss through evaporation and will cause you to feel cold.
(e) Avoid touching metal, especially with wet hands, because it will make you feel colder and may cause frostbite.
(f) Avoid drinking alcoholic beverages because alcohol:-
(i) Interferes with the body's ability to regulate body temperature.
(ii) Affects judgment.
(iii) Can cause blood vessels in the skin to dilate and thus increase heat loss.
(iv) Reduces the body's ability to sense cold, because it depresses the nervous system
(v) Avoid drinking caffeine or smoking, while out in the cold.
(g) Nicotine (from tobacco) and caffeine cause narrowing of the blood vessels in the hands and feet. When vessels are narrowed, less blood can get to those areas causing the hands and feet. to become cold.
It is a burn to the cornea from over exposure to ultraviolet (UV) light. Snow is highly reflective, and can reflect up to 80% incident UV radiation.
(i) Feeling of grit in eyes.
(ii) Increased tear production..
(in) Uncontrolled twitching of eyelids.
(iv) Redness.
(V) Pain.
(vi) Distorted vision (halos, blurriness).
(vii) Light sensitivity.
(viii) Swelling.
(IX) Temporary loss of vision.
(i) Use sunglasses or goggles which are rated for 99-100% UV absorption. They should be of wrap around type, or side shielded with large lenses, that fit close to the face.
(ii) Make sure you have appropriate eye protection, even on overcast days.
(i) If you experience snow blindness, remove yourself from exposure by going into a darkened room or tent.
(ii) Remove contact lenses until your eyes return to normalcy.
(iii) Apply a cool compress to your eyes. Manage pain with over-the-counter medication.
(a) New entrants to high altitude areas comprise mainly tourists, trekkers, mountaineers, porters, workers, soldiers, etc. The entry of these un-acclimatized individuals, along with native highlanders who re-enter high altitudes after moving down or ascending up further from native heights, renders them liable to Acute Mountain Sickness (AMS) at high altitude (HA)-ranging from Benign Acute Mountain Sickness to life threatening or fatal disorders, like acute High Altitude Pulmonary Oedema (HAPO) or High Altitude Cerebral Oedema (HACO)
(i) Decreased partial arterial pressure of oxygen (PaO2). It falls further due to hypoventilation in sleep, leading to tissue hypoxia.
(ii) Cold temperature, high wind velocities, and resultant drop in humidity of air All these lead to dehydration, due to increased insensible loss of water from body.
(iii) Increased ionizing and non ionizing radiations.
(iv) Lowered bariatric pressure, which is directly proportional to high altitude, is a major factor responsible for acclimatization and development of acute mountain sickness.
| Clinical Presentation | Management | Prevention |
| Mild Acute Mountain Sickness Headache with nausea, and dizziness, fatigue during first 12 hrs after ascent to high altitude (3000 M). | Descend 500 M or more, rest and acclimatize; or speed acclimatization. | Ascend at a slow rate; spend a night at an intermediate altitude: avoid overexertion; avoid direct ascent to an altitude of more than 3000 M |
| Moderate Acute Mountain Sickness Moderate to with severe headache marked nausea, dizziness, lassitude, insomnia, and fluid retention at high altitude lasting for 12 hrs or more | Descend 500M or more; if descent is not possible, use a hyperbaric chamber or administer low-flow Oxygen (1-2 lts/min); if descent is not possible, and Oxygen is not available, administer Acetazolamide (250 mg BD). | Ascend at a slow rate, spend a night at an intermediate altitude. avoid overexertion; avoid direct ascent to an altitude of more than 3000 M. |
| High-Altitude Cerebral Oedema (HACO) Acute Mountain Sickness for 24 hrs or more, severe lassitude, mental confusion, ataxia | Initiate immediate descent or evacuation; if descent is not possible, use a portable hyperbaric chamber, administer Oxygen (2-4 Its/min). | Avoid direct transport to an altitude of more than 3000M ascend at a slow rate, avoid overexertion, consider taking |
| High-Altitude Pulmonary Oedemadyspnoea (HAPO) Moist cough, severe weakness, drowsiness, Cyanosis, Tachycardia, Tachypnoea Rales. | Administer Oxygen (4-6 Its/min until condition improves, and then 2-4 Its/min to conserve supplies). Descend as soon as possible with minimal exertion, or use a portable hyperbaric chamber. | Ascend at a slow, graded rate; avoid overexertion; people with earlier episodes should avoid high altitude areas. |
M-meters, PO per orally, IM Intra muscular, IV Intra venous, BD -twice daily, Its litres, q-each quantity, mgmilligrams, hrs-hours.